
Accessible cosmetic dentistry
Lisburn dentist Andrew Wallace argues that a progressive and pragmatic approach to cosmetic dentistry shouldn’t be beyond any willing dental practitioner
When it comes to cosmetic dentistry, dental professionals often focus on providing the patient with an idealised smile. Translating the elements of a beautiful smile into proportions, ratios, rules etc. that can be easily conveyed to a dental technician, easily reproduced, easily taught and remembered1,2.
This rigid adherence to smile design principles may, in some circumstances, result in patients having overtreatment and unnecessarily destructive dentistry3.
Moreover, several studies have shown that the patient’s goal is a natural smile4 and that smiles that correspond to these idealised principles are not actually viewed as any more aesthetic2.
It has been shown that there can be a low correlation between what a clinician believes requires aesthetic correction and the patient’s view5. Less invasive alternatives can offer significant advantages in financial and biologic cost6 and while they may not be viewed by the clinician as the perfect result, they can satisfy the patient particularly if they have been involved in the decision making process7,8. Minor deviations from the ideal are generally not noticed9. Dental appearance can have a significant effect on the patient’s self perception and social interaction 4.
In my view, our goal in aesthetic dentistry should be a smile that the patient views as meeting their aesthetic goals and requires the least amount of tooth tissue loss at a reasonable cost, rather than being able to stand up in front of our peers and present the perfect case or gain accreditation or praise from our colleagues in an organisation or academy. Although some more forward-thinking organisations are now updating their accreditation requirements. A progressive approach 3 where the smile is gradually improved and the patient is allowed to see and assess the improvement before committing to the next stage is a sensible and pragmatic approach.
A patient’s own self-perception and body image can be a motivating factor to attend for cosmetic treatment including cosmetic dentistry4 and patients expect to have and improvement in these post-treatment10. It has been shown most patients do see an improvement in body image and self-esteem after treatment11.
Case study
This 22-year-old man attended the practice as a new patient seeking cosmetic improvement of his upper and lower teeth. His main concern was the crookedness of his upper and lower front teeth and he requested treatment with removable orthodontic appliances if possible. He had not had any form of orthodontics prior to this.
-

- Before treatment: 1a – Full face view
-

- Before treatment: 1b – Lateral profile
-

- Before treatment: 1c-e – Clinical photos used to record the pre-operative condition and to aid in discussion with the patient
-

- Before treatment: 1c-e – Clinical photos used to record the pre-operative condition and to aid in discussion with the patient
-

- Before treatment: 1c-e – Clinical photos used to record the pre-operative condition and to aid in discussion with the patient
Examination was carried out and orthodontic records were taken. Findings: dental class 1 on a skeletal class 2 with moderate upper crowding and moderate lower crowding. Dental midlines were non-coincident and the upper midline was canted to the patient’s right. He had a minimally restored dentition with good oral hygiene.
The treatment options were discussed for anterior alignment of the patient’s teeth, these options included:
- Inman aligner
- Clear aligners
- Fixed appliances with tooth coloured brackets and wires.
Other options discussed included restorative treatment with indirect porcelain restorations as well as the possibility of elective endodontics on at least two teeth.
The advantages and disadvantages of the alternatives were discussed, including the differences in outcomes and where the compromises of each outcome lay.
The patient opted for orthodontics using fixed appliances with clear brackets, as the outcome we expected with these was closer to the patient’s goals.
-

- Figs 2a-d Five month review, clinical photographs are taken at each review to record the progression and aid in the mentoring process
-

- Figs 2a-d Five month review, clinical photographs are taken at each review to record the progression and aid in the mentoring process
-

- Figs 2a-d Five month review, clinical photographs are taken at each review to record the progression and aid in the mentoring process
-

- Figs 2a-d Five month review, clinical photographs are taken at each review to record the progression and aid in the mentoring process
-

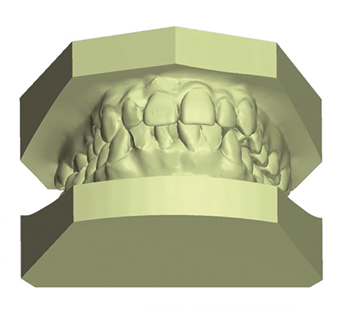
- Figs 3a-d Archwize digital planning
-

- Figs 3a-d Archwize digital planning
-

- Figs 3a-d Archwize digital planning
-
- Figs 3a-d Archwize digital planning
Potential adverse outcomes were detailed, as was the need for slenderising the teeth using IPR and Predictive Proximal Reduction (PPR). The possibility of “black triangles”, the need for edge bonding and lifetime retention were all discussed and the patient agreed to the treatment.
I consulted with an orthodontic mentor about the case and we agreed the treatment objectives were possible using the system, including that the molar cross-bite was related to the angulation of the teeth on the right side and that this could be corrected by uprighting the teeth.
A crowding analysis was carried out and, from this prescription, a predicted outcome was carried out using Archwise software by the laboratory, and these diagrams were used to further relay to the patient the expected outcome. An indirect bracket bonding set-up was carried out by the lab and was fitted at a subsequent appointment.
Treatment took a total of seven-and-a-half months in fixed appliances, the patient was seen at four-weekly intervals where progress was assessed, IPR was carried out as required and the wires changed. Records taken at each appointment included: IPR carried out, wires used, patient complaints and questions. Particular attention was paid to the shape of the teeth during IPR and PPR so that they were detriangulated to reduce the risk of black triangles. Periodically, I consulted with mentors on progress using digital photography and records.
Following debonding of the appliances, the patient had removable retainers fitted immediately, had in surgery zoom whitening shortly after and subsequently fixed bonded wire retainers were made and fitted. Removable retainers were fitted as well and the patient was instructed to wear full-time for three months and night-time only after that.
The patient was unhappy with the shape of the canine teeth and these were reshaped using a single layer of Venus Pearl composite. The patient did not wish to have the incisal edge of the upper left central incisor bonded to address the minor tooth surface loss, even though this was part of the treatment plan.
The outcome of the case is shown in the photographs. The molar and canine relation remains class one with the incisor relation class ı with overjet 3mm and overbite 3mm. The canted midline is corrected and the dental midlines are now coincident.
-

- Figs 4a-d Clinical situation post-treatment showing the final alignment and the aesthetic improvement
-

- Figs 4a-d Clinical situation post-treatment showing the final alignment and the aesthetic improvement
-

- Figs 4a-d Clinical situation post-treatment showing the final alignment and the aesthetic improvement
-

- Figs 4a-d Clinical situation post-treatment showing the final alignment and the aesthetic improvement
Conclusion
We know from the literature that cosmetic dental procedures can improve a patient’s body image and self-esteem11,12 anecdotally. With this young man I noticed a distinct change as his treatment progressed; he started becoming more outgoing, friendly and confident.
With a framework in place identifying clearly what can be treated in general practice and what should be referred to specialist colleagues, along with the mentoring and support from more experienced colleagues and specialists, this sort of treatment is well within the remit of any adequately trained general dentists and is a very rewarding type of dentistry to provide for your patients.
About the author
Andrew Wallace (GDC number 74981), BDS (QUB) MClinDent Prosthodontics (KCL) MFGDP (RCS Eng) is a general dentist with special interest in prosthodontics and orthodontics. Having qualified from Queens University Belfast in 1998, Andrew gained his Master of Clinical Dentistry (MclinDent) in Fixed and Removable Prosthodontics from King’s College London in 2015 and gained full Membership of the Faculty of General Dental Practice (MFGDP) for the Royal College of Surgeons England also in 2015.
Andrew has been a partner in Bachelors Walk Dental 2004 and also works in the multi-award-winning Cranmore dental and implant clinic accepting referrals for restorative dentistry and endodontics. Andrew lectures internationally on cosmetic dentistry, including cosmetic tooth alignment, tooth whitening and is principal trainer in Ireland for the IAS Academy, the group responsible for accrediting professional dental providers of the Inman Aligner and ClearSmile cosmetic orthodontic systems.
Andrew is the current vice president of the European Society of Aesthetic Orthodontics, a key opinion leader for Philips Oral Healthcare and an honorary clinical teacher in King’s College London. Andrew is one of a very small number of dentists acknowledged as an active member of the Irish Academy of Aesthetic Dentistry and is a full member of the British Academy of Cosmetic Dentistry.
References
1. Ward DH. A study of dentists’ preferred maxillary anterior tooth width proportions: comparing the recurring esthetic dental proportion to other mathematical and naturally occurring proportions. J Esthet Restor Dent. Blackwell Publishing Inc; 2007;19(6):324–37–discussion338–9.
2. Schabel BJ, Franchi L, Baccetti T, McNamara JA Jr. Subjective vs objective evaluations of smile esthetics. Am J Orthod Dentofacial Orthop. Elsevier; 2009 Apr;135(4):S72–9.
3. Qureshi A. Who needs Veneers [Web]. Journal Of Cosmetic Dentistry. [Jun 25 2011]. pp. 85–94. From: www.towniecentral.com/MessageBoard/UserUploads/Attachments/111958_Qureshi_939.pdf
4. Davis LG, Ashworth PD, Spriggs LS. Psychological effects of aesthetic dental treatment. J Dent. 1998 Sep;26(7):547–54.
5. Tortopidis D, Hatzikyriakos A, Kokoti M, Menexes G, Tsiggos N. Evaluation of the relationship between subjects’ perception and professional assessment of esthetic treatment needs. J Esthet Restor Dent. 2007;19(3):154–62–discussion163.
6. Burke FJ, Kelleher M, Wilson N. Introducing the concept of pragmatic esthetics, with special reference to the treatment of tooth wear. Journal of Esthetic and …. 2011.
7. Nalbandian S, Millar BJ. The effect of veneers on cosmetic improvement. Br Dent J. Nature Publishing Group; 2009 Jul 25;207(2):E3–E3.
8. Spear FM. Esthetic Correction of Anterior Dental Malalignment: Conventional versus Instant (Restorative) Orthodontics. Journal of Esthetic and Restorative Dentistry. Blackwell Publishing Ltd; 2004;16(3):149–62.
9. Kokich VO, Asuman Kiyak H, Shapiro PA. Comparing the Perception of Dentists and Lay People to Altered Dental Esthetics. J Esthet Restor Dent. Blackwell Publishing Ltd; 1999;11(6):311–24.
10. Pabari S, Moles DR, Cunningham SJ. Assessment of motivation and psychological characteristics of adult orthodontic patients. American Journal of Orthodontics and Dentofacial Orthopedics. 2011 Dec;140(6):e263–72.
11. Varela M and García-Camba JE. Impact of orthodontics on the psychologic profile of adult patients: a prospective study. American Journal of Orthodontics and Dentofacial Orthopedics: 1995 108(2), 142–148.
12. Sarin S, Gilbert D and Asimakopoulou K. (2014). Why simple aesthetic dental treatment in general practice does not make all patients happy. British Dental Journal, 216(12), 681–685.
You must be logged in to post a comment.