Socket preservation

Dr Laura Fee looks at the various techniques and materials available for the purposes of socket preservation post extraction
Socket preservation is a procedure that reduces bone and soft tissue loss after tooth extraction. It is performed immediately after tooth extraction. It has been found that ridge preservation procedures following tooth extraction result in greater orofacial dimension of bone when compared with cases where no ridge preservation procedures are completed1.
Socket preservation is indicated as tooth extraction can have a significant impact on the facial bone height2. After eight weeks of healing there is, on average, 20 per cent horizontal resorption and a 50 per cent reduction of vertical bone wall height3.
Immediate implant placement does not counteract alveolar ridge modelling after tooth extraction4. Socket preservation compensates for the biologic resorption of the facial bone wall. It aids implant placement and can reduce the need for later bone augmentation. By reducing marginal bone loss on adjacent teeth and accelerating bone formation it can increase implant survival and success3.
Socket preservation should be considered when:5
- Implant placement needs to be delayed for patient or site-related reasons
- In situations where implant placement needs to be postponed for more than six months
- Future fixed partial denture pontic site is planned.
Post-extraction healing
The alveolar process resorbs after tooth extraction, significantly impacting oral rehabilitation with dental implants and other types of prosthesis. Following extraction, the blood clot forms and defensive cells such as polymorphonucleocytes migrate into the socket to help fight infection.
Bundle bone lines the socket with remnants of the periodontal ligament. Coagulate necrosis occurs and a provisional matrix is formed with newly-formed blood vessels along with immature collagen fibres. By day seven, the bundle bone begins to break down and osteoclastic activity creates gaps within this bone. New blood vessels access the socket and newly-woven bone forms around angiogenesis. At day seven to 14, the bundle bone lining is removed6. By day 14 the bone is more mature. The removal of bundle bone has significant implications for implant stability2. Bundle bone resorption causes a loss of height and width of buccal bone. Over 12 months it has been shown that 50 per cent of horizontal width of the ridge disappears. Within the first three months two-thirds of that total reduction has already taken place7.
Biomaterials for socket grafting8
The choice of bone grafting material should assure the long-term stability of the bone volume and should be based on solid documentation in the literature. There is currently not enough data available to indicate superiority of one method or material over another9. The complete regeneration of dehiscence and fenestration-type defects cannot be predictably accomplished regardless of which grafting protocol is implemented1.
Autograft: Bone from same individual which predictably accelerates new bone formation. Disadvantage is unpredictable resorption and donor site morbidity and resorptive tendency changes with harvesting technique10.
Allograft: Bone from same species but another individual. These include free frozen bone, freeze-dried bone allograft, demineralised freeze-dried bone allograft and deproteinised bone allograft. This is an osteoconductive material. Disease transmission has been reported in the past11.
Xenograft: Material of biologic origin but another species such as animal, corals or calcifying algae. No reports of disease transmission. Surface characteristics of xenografts are dependent on preparation method. This is an osteoconductive material as all proteins are removed so there is no osteoinductive potential12.
Alloplast: Material from synthetic origin such as calcium phosphates, glass ceramics and polymers. The biggest challenge for alloplastic materials has been reproducing the surface characteristics of biologically-derived materials. The degradation, however, may be modified according to our clinical indications by changing the material’s chemical structure12.
Dentists should strive to use a well-documented material with a low substitute rate which results in less horizontal and vertical bone resorption. The use of a barrier membrane is indicated whenever a particulate material is used as it encourages increased bone fillı. Resorbable collagen membranes such as Jason Membrane demonstrate good cell occlusiveness, good handling properties and have a low susceptibility to complications13.
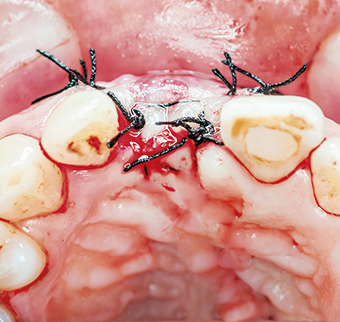
Socket sealing14
- Primary closure after elevating and mobilising a full-thickness mucoperiosteal flap
- Free gingival graft – autogenous
- Dermal allografts
- Collagen matrix xenografts.
Socket sealing has shown less horizontal and vertical bone resorption when used with Bio-Oss collagen15.
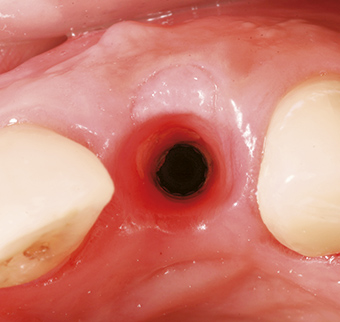
The ideal healing time before implant placement is reported as being six to nine months to allow for adequate healing of bone substitutes materials16.
Treatment alternatives5
- Immediate implant placement if intact socket walls, thick facial bone wall, thick gingival biotype, no acute infection and good primary stability
- Early implant placement usually at six to eight weeks in the aesthetic zone
- Conventional implant placement at three months post-extraction
- Socket preservation – in cases where implant placement needs to be delayed due to patient or site-related factors. This is beneficial in situations where implant placement needs to be postponed for more than six months.
| Table 1. Alveolar ridge preservation17 |
||
|---|---|---|
| HORIZONTAL | VERTICAL | |
| Socket preservation | 1.31mm | 0.91mm |
| Unassisted socket healing | 1.54mm | 1.12mm |
Is it evidence-based? (Table 1)
Socket preservation does not increase implant survival or success. It has been shown that implant placement is always possible whether the socket has been preserved or not5. Further bone augmentation has been shown to be needed in 9.9 per cent of socket preserved cases compared with 20.8 per cent unassisted socket healing casesı4. According to the study completed by Mardas, socket preservation reduces the marginal bone loss by 0.039mm compared with unassisted socket healing. Autograft results in faster bone healing compared with any other bone substitute material such as Bio-Ossı8. Araujo et al showed significant preservation of the facial bone volume with Bio-Oss Collagen at six months19.
However, socket preservation does not accelerate bone formation.
A CBCT clinical study examining 28 patients with single tooth flapless extractions compared DBBM/collagen grafts versus a blood clot in sockets alone. It was shown that by placing a graft into a socket that the amount of horizontal resorption can be reduced but it will have no impact on the vertical change of the buccal bone wall. Bundle bone on the facial wall resorbs irrespective of ridge maintenance procedures which can have implications in the aesthetic zone. This necessitates a second bone grafting procedure at the time of implant placement20.
Socket preservation in growing individuals21
There is limited evidence concerning socket preservation in growing individuals. Sandor completed socket preservation in 21 patients with a mean age of 13 years old. The results of this study showed that 83 per cent of the post-traumatic cases also needed simultaneous grafting with implant placement. Also 6.5 per cent of sockets preserved after the extraction of ankylosed primary molars needed re-grafting.


Conclusions
Most of the resorptive changes of the buccal bone wall have already taken place at eight weeks. Clinical intervention is needed for ridge maintenance as ridge alteration occurs rapidly decreasing its bone volume. Socket preservation results in a greater orofacial dimension of the alveolar ridge than unassisted socket healing.
Bone substitute materials and/or barrier membranes do not accelerate bone healing in extraction sockets. Implant placement must be delayed for a minimum of six months.
Socket preservation may be indicated if implant placement has to be postponed for more than six months after tooth extraction. No superior technique or biomaterial has been identified. However, a bone substitute material with a low substitute rate is recommended.
About the author
Dr Laura Fee graduated with an honours degree in Dental Science from Trinity College, Dublin in 2010. Laura is currently completing a Masters in Dental Implants and works in private practice in Dublin.
References
1. Chen ST. Clinical and Esthetic Outcomes of Implants Placed in Postextraction Sites. Int J Oral Maxillofac Implants 2009; 24(Suppl):186-217
2. Araujo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol 2005 Feb; 32(2): 212-8
3. Chappuis V, Engel O, Reyes M, Shahim K, Nolte LP, Buser D.Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res 2013 Dec; 92(12 Suppl):195S-201S
4. Clementini M, Tiravia L, De Risi V, De Sanctis M. Dimensional Changes after immediate implant placement with or without simultaneous regenerative procedures: A systematic review and meta-analysis. J Clin Periodontol June 2015 42(7) 599-702
5. Martin WC, Morton D. The Influence of Restorative Procedures on Esthetic Outcomes in Implant Dentistry: A Systematic Review. Int J Oral Maxillofac Implants 2014; 29(Suppl):142-154
6. Cardoropoli G, Araujo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. J Clin Periodontol Sept 2003; 30(9): 809-818
7. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodontics Restorative Dent. 2003 Aug; 23(4): 313-23
8. Chen et al. IJOMI 2014, Atieh et al. Ways of keeping enough jaw bone to allow for dental implants after teeth have been taken out. Cochrane Libr Published May 2015
9. ITI Group 1 Consensus Statements: Consensus Statements and Recommended Clinical Procedures Regarding Contemporary Surgical and Radiographic Techniques in Implant Dentistry. Bornstein MM et al. IJOMI 2014
10. Miron RJ, Hedbom N, Saulacic Y, Zhang A, Sculean D, Bosshardt E and Buser D. Osteogenic Potential of Autogenous Bone Grafts Harvested with Four Different Surgical Techniques. J Dent Res 2011 90:1428
11. Boyan BD, Ranly DM, Mc Millan J, Sunwoo M, Roche K et al. Osteoinductive ability of human allograft formulations. J
Periodontol 2006;77:1555-1563
12. Jensen SS, Broggini N, Hjorting-Hansen E, Schenk R, Buser D. Bone healing and graft resorption of autograft, anorganic bovine bone and – ticalcium phosphate. A histologic and histomorphometric study in the mandibles of minipigs. Clinical Oral Implants Research. 2006; 17(3):237-243
13. Von Arx T et al. Membrane Durabillity and Tissue Response of Different Bioresorbable Barrier Membranes: A Histologic Study in the Rabbit Calvarium. Int J Oral Maxillofac Implants 2005; 20:843-853
14. Thalmair T, Hinze M, Bolz W et al. The healing of free gingival autografts for socket-seal surgery: a case report. Eur J Esthet Dent 2010; 5(4): 358-368
15. Jung RE, Hurzeler MB, Thoma DS, Khraisat A. Local tolerance and efficiency of two prototype collagen matrices to increase the width of keratinized tissue. Journal of Clinical Periodotology 2011; 38(2):173-179
16. Mardas N, Trullenque-Eriksson A, MacBeth N, Petrie A, Donos N. Does ridge preservation following tooth extraction improve implant treatment outcomes: a systematic review: Group 4: Therapeutic concepts and methods. Clin Oral Implants Res. 2015 Sep; 26 Suppl 11:180-201
17. Willenbacher et al. The Effects of Alveolar Ridge Preservation: A Meta-Analysis. Clinical Implant Dentistry and Related Research. Doi:10.111/cid.12364
18. Carmagnola D, Adriaens P, Berglundh T Clin. Healing of human extraction sockets filled with Bio-Oss. Clinical Oral Implants Research 14, 137-143
19. Araujo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clinical Oral Implants Research. 2009; 20(6): 545-549
20. Araujo MG, da Silva JC, de Mendonca AF, Lindhe J. Ridge alterations following grafting of fresh extraction sockets in man. A randomized clinical trial. Clin Oral Implants Res. 2015 Apr; 26(4):407-12
21. Sandor GK, Kainulainen VT, Queiroz JO, Carmichael RP, Oikarinen KS. Preservation of ridge dimensions following grafting with coral granules of 48 post-traumatic and post-extracction dento-alveolar defects. Dent Traumatol. 2003 Aug; 19(4): 221-7
The image featured above, and in listings for this article is used courtesy of r.classen / shutterstock.com
You must be logged in to post a comment.